

The fovea is a 1.5 mm pit at the very center of your retina, and its center holds about 199,000 cone photoreceptors per square millimeter, the densest patch anywhere in your visual system.1,5 It delivers your sharpest central detail and your most precise color discrimination, from the words on this page to the face across the room. The macula surrounds and protects it; the rest of the retina supports it; but only this tiny depression delivers what doctors call high-acuity vision.
When the fovea is healthy, you do not notice it. When it is damaged, even slightly, the world dims at its center while your peripheral vision stays intact. That is why conditions like macular degeneration, diabetic macular edema, and macular holes are so disabling: they attack the one square millimeter of retina that does almost all the visual work.
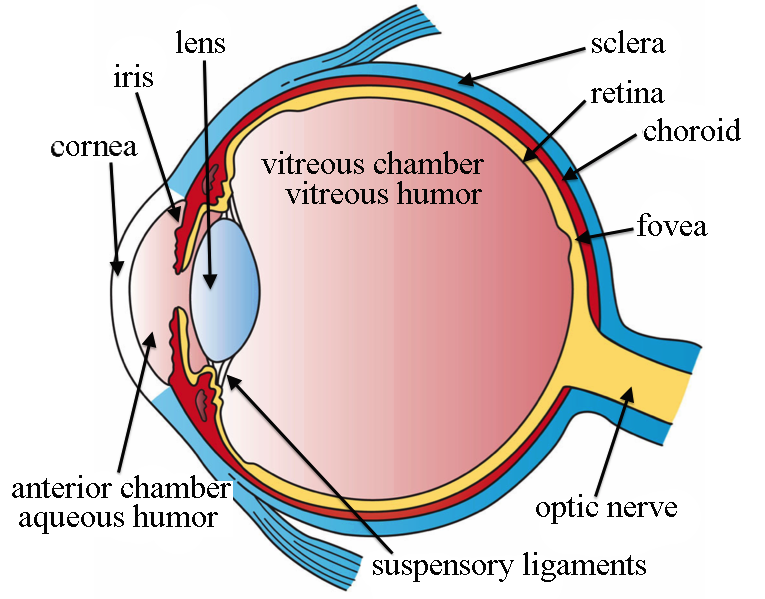
Source: Wikipedia Commons
This article covers where the fovea sits inside the eye, the anatomy that makes it so precise, the conditions that damage it, and the daily habits that help protect it.
Anatomy of the Fovea
The fovea centralis is a 1.5 mm depression at the center of the macula lutea, which itself sits at the center of the retina on the posterior pole of the eye, directly behind the lens and pupil.1,3 Knowing the nesting matters: fovea inside macula inside retina, all aligned on the visual axis.
Size and Structure
The fovea is about 1.5 mm across.2,4 At its very center is the foveola, a smaller floor about 0.35 mm in diameter that contains the thinnest, most tightly packed cone photoreceptors in the entire eye.2,4 The foveola is the seat of the very sharpest vision within the already sharp fovea.
A unique feature of the foveal pit is that all the other retinal cell layers are displaced outward, creating a thin window so light can reach the cones with as little scattering as possible. This structural shift is part of what makes the fovea optically privileged.
Cone Density and the Absence of Rods
Cone cells handle color and fine detail. Rod cells handle low-light and peripheral vision. The central fovea contains only cones and virtually no rods.1,2 Rods cluster in the surrounding retina, not in the central pit.
At the very floor of the fovea, peak cone density averages about 199,000 cones per square millimeter, the highest concentration anywhere in the human visual system, though the figure varies between individuals.5 Foveal cones are also narrower and more elongated than cones elsewhere in the retina, which lets them pack more densely without overlapping their light-sensing tips.
Blood Supply
The central fovea, called the foveal avascular zone, contains no retinal blood vessels.1,2 Foveal photoreceptors receive their oxygen and nutrients from the choroid, the dense vascular layer that sits behind the retinal pigment epithelium. This avascular design avoids scattering light through blood vessels in the very spot where optical clarity matters most. It also makes the fovea uniquely vulnerable: it depends entirely on choroidal circulation, and any disruption shows up quickly as blurred or distorted central vision.
What Does the Fovea Do?
The fovea is the part of the retina that produces maximum visual acuity. To see anything sharply, your eye must focus that image onto the fovea.1,3 Activities like reading, threading a needle, recognizing a face, and judging detail at distance all depend on foveal vision.
Foveal vision covers only the central two degrees of your visual field, about twice as wide as your thumbnail held at arm's length. Everything outside that narrow cone is peripheral vision, which is fast, motion-sensitive, and far less detailed.
This is why your eyes are constantly moving. Each rapid shift of gaze, called a saccade, steers the fovea toward the next thing your brain wants to examine. You are not scanning a sentence with your whole retina; you are sweeping the fovea word by word.
Conditions That Damage the Fovea
A range of eye conditions can injure the fovea or the macula that surrounds it. Because the fovea controls central vision, damage here causes blurry, distorted, or missing vision at the spot you are looking at, even when the rest of your visual field stays clear.
Age-Related Macular Degeneration (AMD)
Age-related macular degeneration is a leading cause of vision loss among older adults in the United States. CDC estimates suggest about 19.8 million Americans age 40 and older have AMD, including roughly 1.5 million with vision-threatening disease.6 AMD damages the macula and, in advanced stages, the fovea, producing central vision loss with intact peripheral vision.
AMD comes in two forms: dry (gradual thinning of the macula) and wet (abnormal new blood vessels grow under the retina and leak fluid or blood). Wet AMD causes faster vision loss and is treated differently from dry AMD.
Macular Hole
A macular hole is a small break in the tissue at the center of the macula, often right at the fovea.7 Macular holes usually develop with age as the vitreous gel inside the eye pulls away from the retina. They are not the same as age-related macular degeneration.
Early symptoms are blurry or wavy central vision. As the hole opens, a dark spot or gap appears in the center of sight. Peripheral vision typically remains intact.
Branch Retinal Vein Occlusion (BRVO)
Branch retinal vein occlusion occurs when one of the smaller veins draining the retina becomes blocked.8 Blood and fluid can leak into the retina, often causing macular swelling that blurs central vision. Without an intact blood supply, retinal and foveal cells can eventually die.
Choroidal Neovascular Membranes (CNVM)
Choroidal neovascular membranes are abnormal new blood vessels that grow from the choroid into the space beneath the retina. They are most often associated with advanced wet macular degeneration.6 When these vessels leak or bleed, they damage the overlying retina and fovea and cause sudden central vision loss.
Cytomegalovirus (CMV) Retinitis
CMV retinitis is a serious viral infection of the retina that most often affects people with weakened immune systems, including those with advanced HIV or who are taking immunosuppressive medications.15 Symptoms include the slow onset of floaters, blurred vision, and sometimes central vision loss if the infection reaches the macula or fovea.
Diabetic Retinopathy
Diabetic retinopathy is damage to the retinal blood vessels caused by long-term high blood sugar.10 Vessels can leak, become blocked, or trigger the growth of abnormal new vessels. When fluid leaks into the macula, the resulting diabetic macular edema is the most common cause of vision loss in people with diabetes.
Histoplasmosis (Presumed Ocular Histoplasmosis Syndrome)
Histoplasmosis is a lung infection caused by inhaling spores of the fungus Histoplasma capsulatum. Experts think the spores can travel from the lungs to the eye, leaving small scars in the choroid that can later trigger abnormal blood vessel growth and vision loss.14 The result is presumed ocular histoplasmosis syndrome (POHS), which can damage the macula and fovea.
Macular Edema
Macular edema is fluid buildup and swelling in the macula. It typically causes blurry vision and washed-out colors.9 Common causes include diabetic retinopathy, retinal vein occlusion, age-related macular degeneration, uveitis, and the aftermath of certain eye surgeries.
Retinitis Pigmentosa
Retinitis pigmentosa is a group of inherited disorders that progressively damage the photoreceptors of the retina.11 Most people first lose night vision and peripheral vision; many eventually lose central vision and color vision as the disease reaches the macula.
Retinal Detachment
Retinal detachment is when the retina separates from the back of the eye. It is a medical emergency that requires immediate care to avoid permanent vision loss.13 Early symptoms include a sudden burst of floaters, flashes of light, and a shadow or dark curtain creeping across your vision.
Retinoblastoma
Retinoblastoma is a rare pediatric eye cancer that develops in the retina and most often appears in children under five.16 It can spread to other parts of the eye and, if untreated, beyond the eye. A white reflection in the pupil seen in photos or under bright light is a common early sign and a reason to see a pediatric ophthalmologist promptly.
Stargardt Disease
Stargardt disease, also called juvenile macular dystrophy, is an inherited condition that damages the photoreceptors of the macula in children and young adults.12 Unlike age-related macular degeneration, central vision loss usually begins in childhood or adolescence.
Protecting Your Fovea
The fovea cannot be repaired once it is destroyed, but several everyday habits help protect it across a lifetime. The most important measures are simple and well supported.
- Get a dilated eye exam on the right schedule for your age and risk. Adults without symptoms or known eye disease should follow an age-based exam schedule that gets more frequent as you get older. People with diabetes, a family history of AMD, or other retinal risk factors often need more frequent exams, sometimes annually, based on what their eye doctor recommends.10 Dilated exams let your eye doctor see the macula and fovea directly and catch problems before symptoms appear.
- Control diabetes, blood pressure, and cholesterol. The most common preventable causes of foveal damage are diabetic macular edema and retinal vein occlusions, both of which are driven by vascular disease.10 Stable blood sugar and blood pressure protect the small vessels that feed the retina.
- Do not smoke. Smoking is one of the strongest modifiable risk factors for age-related macular degeneration. Quitting at any age reduces that risk.6
- Wear UV-blocking sunglasses outdoors. Some studies link long-term, unprotected UV exposure with an increased risk of AMD. Look for sunglasses labeled 99 to 100 percent UVA/UVB protection or "UV400."
- Eat for retinal health. Diets rich in dark leafy greens, colorful vegetables, and oily fish provide lutein, zeaxanthin, and omega-3 fatty acids, which are concentrated in the macula. People with intermediate AMD or late AMD in one eye may benefit from AREDS2 supplements, but these should be started only on the advice of an eye doctor and are not a general prevention strategy.6
- Pay attention to sudden vision changes. New distortion, a dark spot in the center of vision, flashes, a shower of floaters, or a curtain across your vision are all signs of retinal or foveal problems that need same-day evaluation.
When to See a Doctor
See your eye doctor promptly if you notice any of the following:
- New blurring, distortion, or a missing patch in your central vision
- Straight lines, like door frames or window grids, that look wavy or bent
- A sudden increase in floaters or new flashes of light
- A shadow, curtain, or dark area drifting across your field of vision
- Any sudden, painless loss of vision in one eye
The last three symptoms can signal retinal detachment or a vitreous hemorrhage and warrant emergency evaluation, not a routine appointment.
Why Routine Eye Exams Matter
Many foveal conditions, including early AMD, mild diabetic retinopathy, and small macular holes, cause few symptoms in their earliest stages. A comprehensive dilated eye exam lets your eye doctor inspect the macula and fovea directly. Optical coherence tomography (OCT), a non-invasive scan that produces a cross-section image of the retina, is often used to measure macular thickness, detect fluid, and follow conditions over time.9
Treatment Options for Foveal Disease
Treatment depends on the cause of damage and how far it has progressed. The most common options include:
- Anti-VEGF injections. Injectable medications that block abnormal blood vessel growth and reduce leakage. They are first-line treatment for diabetic macular edema, wet age-related macular degeneration, macular edema after retinal vein occlusion, and choroidal neovascularization from ocular histoplasmosis syndrome.17
- Complement-inhibitor injections for geographic atrophy. For some people with geographic atrophy (the advanced form of dry AMD), eye injections that target the complement immune pathway can slow the growth of atrophic lesions. They do not restore lost vision, and the decision to use them involves an individualized risk-benefit discussion with a retina specialist.6
- Laser surgery. Focal laser is used in some cases of diabetic macular edema or to treat leaking vessels outside the foveal center. Anti-VEGF injections have largely replaced laser as first-line treatment for most macular swelling.9
- Vitrectomy. A surgical procedure used most often for macular hole repair, advanced diabetic retinopathy, and certain retinal detachments. In macular hole surgery, the vitreous gel is removed and replaced with a gas bubble that holds the hole closed while it heals.7
- AREDS2 supplements. A specific formulation of lutein, zeaxanthin, vitamin C, vitamin E, zinc, and copper can slow the progression of intermediate AMD or late AMD in one eye in carefully selected patients.6 AREDS2 is not a treatment for early AMD and is not a substitute for routine eye care.
Summary
The fovea is a 1.5 mm pit at the center of the retina. At its center, peak cone density reaches about 199,000 cones per mm², and photoreceptors are supplied by the choroid rather than the retinal vessels. It delivers your sharpest central vision and your most precise color discrimination for tasks like reading, driving, and recognizing faces, and it covers only the central two degrees of your visual field.
A range of conditions, from age-related macular degeneration and macular holes to diabetic macular edema and retinal detachment, can damage the fovea and cause central vision loss while peripheral vision remains intact. Most of these conditions are treatable when caught early, especially with anti-VEGF injections and timely surgery.
Regular dilated eye exams, well-controlled diabetes and blood pressure, no smoking, UV-blocking sunglasses, and a retina-friendly diet are the best ways to protect the fovea across a lifetime. Any sudden distortion, central blur, flashes, or curtain across your vision is a reason to see your eye doctor the same day.
Frequently Asked Questions on the Fovea
Is the fovea the same as the blind spot?
No. The fovea is the area of the retina with the highest visual acuity. The blind spot is where the optic nerve leaves the eye at the optic disc, and it contains no photoreceptors of any kind. You do not normally notice the blind spot because your brain fills it in.
What happens to your vision if the fovea is damaged?
Damage to the fovea causes reduced visual acuity in the center of your vision, often along with trouble seeing colors and fine details. Peripheral vision usually stays intact, which is why people with foveal damage can often still walk, find their way around a room, and detect motion, even when they can no longer read print or recognize faces.
Can you see without the fovea?
Yes, but not sharply. Some people are born with an underdeveloped or absent foveal pit, a condition called foveal hypoplasia, which is associated with reduced visual acuity from birth.18 People who lose foveal function later in life, from AMD or other macular disease, retain their peripheral vision but lose central detail.
How does an eye doctor check the fovea?
The two main tools are a dilated fundus exam, in which the eye doctor looks directly at the macula and fovea with a special lens, and optical coherence tomography (OCT), a non-invasive scan that produces a cross-section image of the retina layer by layer.9 OCT can detect macular swelling, holes, and thinning before they cause noticeable symptoms.

