

What Is Papilledema?
Papilledema is swelling of the optic nerve where it enters the back of the eye, caused by increased pressure inside the skull. Both eyes are usually affected. It is different from a naturally large optic nerve, which is harmless, and different from Normal-Tension Glaucoma, where the nerve is damaged but not swollen. Because papilledema can signal a brain tumor, bleeding, infection, or dangerously high pressure inside the head, it is treated as a medical emergency until those causes are ruled out.
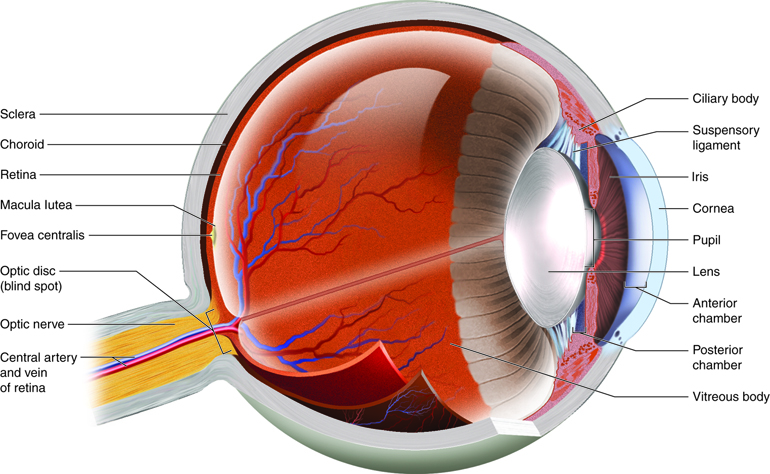
The optic nerve (also called the second cranial nerve or CNII) transmits visual information from the eyes to the brain. When pressure inside the skull rises, it pushes against the back of the optic nerve. The result is visible swelling at the optic disc, the spot where the nerve meets the retina.
When Is a Swollen Optic Nerve an Emergency?
Treat papilledema as urgent if you have any of the following:
- Sudden or recurring blurred vision
- Double vision or brief "blackouts" in vision
- Severe headache, especially with nausea or vomiting
- New pulsating sounds in the ears
- A clinician telling you there is optic nerve swelling on exam
Papilledema can be linked to brain swelling, bleeding, tumors, infection, or dangerously increased intracranial pressure. Get evaluated the same day, in the emergency room or by a neuro-ophthalmologist.
Listen In Q&A Format
Papilledema: Swollen Optic Nerve
Vision Center Podcast
Is It Papilledema, a Large Optic Nerve, or Glaucoma?
When an eye doctor tells you your optic nerve looks enlarged, the cause falls into one of three buckets. Only one is a true emergency.
| Finding | What it means | Is it urgent? |
|---|---|---|
| Naturally large optic nerve | Some people are born with bigger optic nerve heads and "cups." Vision is stable, no nerve fibers are damaged. | No. Routine monitoring only. |
| Normal-Tension Glaucoma (NTG) | The optic nerve is damaged even though eye pressure stays in the normal range. Vision loss is slow and painless, starting in the peripheral field. | Not an emergency, but needs glaucoma treatment to prevent further damage. |
| Papilledema | The optic nerve is actually swollen because pressure inside the skull is too high. Caused by tumors, bleeding, infection, or idiopathic intracranial hypertension. Usually affects both eyes. | Yes. Go to the ER or see a neuro-ophthalmologist the same day. |
A dilated eye exam and OCT help confirm whether the disc is truly swollen. If papilledema is suspected or confirmed, urgent brain imaging (typically MRI with MRV) is used to look for an underlying cause before a lumbar puncture is performed. If your doctor saw true swelling, not just a large nerve, the workup begins immediately.
Common Questions About Swollen and Enlarged Optic Nerves
Can you have glaucoma with normal pressure?
Yes. Normal-Tension Glaucoma damages the optic nerve at normal eye pressures, likely from poor blood flow to the nerve or unusual nerve sensitivity. It is different from papilledema, where the nerve is swollen because of pressure inside the skull, not the eye.
Can it be normal to have a large optic nerve?
Yes. Some people are born with naturally larger optic nerve heads, called physiologic cupping. It is harmless and does not cause symptoms, but your eye doctor will monitor it to rule out glaucoma.
What is Stage 1 early papilledema?
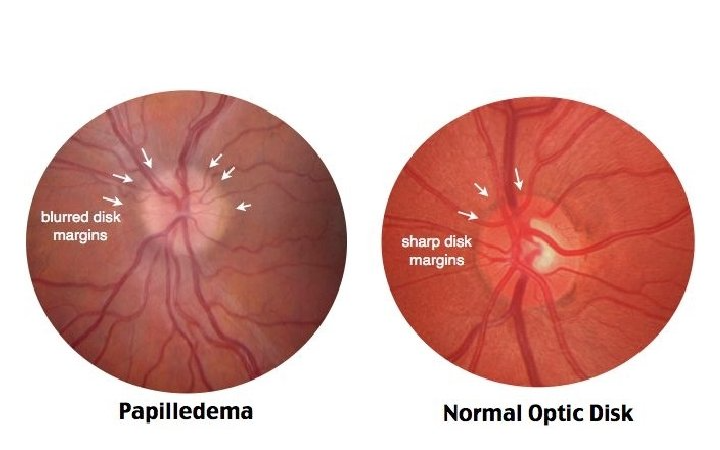
Stage 1 (Frisén grade 1) is mild swelling at the edges of the optic disc, with the disc margin starting to blur. There is no visible elevation of the nerve and usually no symptoms. It is detected on a dilated eye exam or OCT.
Can a swollen optic nerve be nothing?
No. True swelling is never normal. But some doctors use the word "swollen" loosely to describe a naturally large or full-looking nerve that is not actually swollen. OCT and a dilated exam tell the difference, so push for a clear answer if the wording is ambiguous.
How Papilledema Differs From Optic Disc Edema
Papilledema and optic disc edema both involve a swollen-looking optic disc, but the causes are different:
- True papilledema: Disc swelling caused specifically by increased pressure inside the skull, often from a tumor, infection, or idiopathic intracranial hypertension
- Optic disc edema: True swelling of the disc from a local cause in the eye or optic nerve, such as optic neuritis, ischemic optic neuropathy, or retinal vein occlusion
- Pseudopapilledema: A separate condition where the disc looks elevated but is not actually swollen, often from buried optic disc drusen or a naturally crowded disc
Papilledema commonly affects your peripheral vision and spares central vision until late. Optic disc edema from local optic nerve causes often affects central vision first.
Signs and Symptoms of Papilledema
Transient visual obscurations (TVOs) are the most distinctive early symptom of papilledema: brief blackouts in vision lasting seconds, triggered by standing up, bending over, or coughing. Many patients have no vision changes at first and instead notice signs of raised intracranial pressure: a headache that is worse on waking, nausea, and vomiting.
Vision Symptoms
- Transient visual obscurations (TVOs): Brief blackouts in vision lasting seconds, triggered by positional changes such as standing up, bending over, or coughing
- Blurred or double vision (diplopia)
- Decreased peripheral vision; central vision is preserved until late in the disease
- In severe cases: decreased visual acuity, impaired color perception, complete vision loss
Pressure Symptoms (Raised ICP Signs)
- Headache that is worse on waking and worsens when lying flat or straining
- Nausea and vomiting, sometimes projectile (sudden and forceful, without warning nausea)
- Pulsatile tinnitus: A rhythmic whooshing or thumping in one or both ears that syncs with the heartbeat
- Sixth nerve palsy: one eye may drift inward, causing horizontal double vision, because the sixth cranial nerve takes a long path inside the skull that makes it vulnerable to rising pressure
- In emergencies: Cushing's Triad (slowing heart rate, irregular breathing, and a widening pulse pressure)
Papilledema itself does not cause eye pain, but the underlying headache usually does. If your eye hurts when you move it, the cause is more likely optic neuritis, a different condition with a different workup.
What Causes Papilledema?
Most cases of papilledema fall into one of three categories: a mass inside the skull (tumor, abscess, hemorrhage), a problem with cerebrospinal fluid flow (hydrocephalus, venous thrombosis), or idiopathic intracranial hypertension. Infections and head trauma make up the remainder.
Specific known causes include:
- Brain tumor
- Brain abscess
- Head trauma
- Brain aneurysm
- Stroke
- Hydrocephalus
- Severe high blood pressure
- Brain hemorrhage
- Cerebral edema
- Craniosynostosis
- Meningitis
- Encephalitis
- Cerebral venous thrombosis (CVT)
Optic pathway gliomas (slow-growing tumors on the optic nerve) can cause swelling of one optic disc from local pressure on the nerve itself. In some cases, especially when the tumor blocks cerebrospinal fluid flow or causes hydrocephalus, it can also raise pressure inside the skull and produce true papilledema.
When no structural cause is found, the condition is called idiopathic intracranial hypertension (IIH) or pseudotumor cerebri. IIH mimics a brain tumor on symptoms without showing one on imaging.
Medications That Can Trigger Papilledema
Medications most commonly linked to papilledema and IIH include tetracycline antibiotics (doxycycline, minocycline), isotretinoin (Accutane), high-dose vitamin A, corticosteroids during withdrawal, lithium, and growth hormone. Less commonly, sulfa antibiotics and some IV anti-hypertensive drugs (nitroprusside, hydralazine) have been reported.
If you are on any of these drugs and develop headaches, vision changes, or pulsatile tinnitus, tell your doctor about the medication when you ask for an exam. Stopping the triggering drug early gives you the best chance of recovery, but drug-induced papilledema still needs a prompt eye exam and ongoing vision monitoring. Vision loss has been reported when the medication is not stopped in time.
Risk Factors
Papilledema is rare, but the risk concentrates in one group: women of childbearing age (15 to 44) with obesity. This population is up to 20 times more likely to develop idiopathic intracranial hypertension, the most common cause of papilledema without a structural lesion.
IIH occurs in roughly 1 out of 100,000 Americans overall. Sudden weight gain (at least 5 to 15% of your body weight in a short window) is an additional trigger for IIH.
How Papilledema Is Diagnosed
The diagnostic anchor is a dilated fundus exam and optical coherence tomography (OCT), which together confirm whether the disc is truly swollen and to what degree. If papilledema is suspected, urgent brain imaging (typically MRI with MRV) follows to look for a mass or a blood clot in a brain vein. A lumbar puncture (spinal tap) is done after imaging confirms it is safe. Your doctor will also collect medical history, vital signs, height, and weight to identify risk factors for IIH and other causes of raised intracranial pressure.
Additional tests used to confirm papilledema and find its cause include:
- Perimetry (visual field testing)
- Fluorescein angiography
- B-scan ultrasonography
- Computed tomography (CT) scan
- Magnetic resonance imaging (MRI)
- Magnetic resonance venography (MRV)
- Stereo color photography of the optic disc
- Lumbar puncture (spinal tap) to measure CSF pressure
If papilledema is confirmed, an eye specialist uses the Frisén scale to grade severity, from grade 1 (subtle blurring at the disc margins) to grade 5 (severe swelling with hemorrhages and obscured retinal vessels). The grade guides treatment urgency and follow-up frequency.
Complications of Papilledema
The headline complication is permanent vision loss. Sustained pressure on the optic nerve damages nerve fibers, and once the nerve atrophies (becomes pale and shrunken), vision does not return.
Additional complications depend on the underlying cause. Raised intracranial pressure from a brain hemorrhage, a ruptured aneurysm, or a stroke can cause direct brain injury, herniation, or death if pressure is not brought down quickly. A brain abscess can lead to meningitis, venous thrombosis, and sepsis. Some causes require immediate treatment to prevent death.
Is Papilledema Reversible?
Often, if treated early. When the underlying cause of raised intracranial pressure is treated promptly, vision frequently improves. Recovery depends on the cause, how severe the swelling was, and whether the optic nerve has already been damaged. Once the swelling has progressed to optic atrophy (a pale, shrunken nerve), the vision loss is permanent.
The success of treatment depends on accurate diagnosis. If your doctor does not identify the exact cause of the raised intracranial pressure, symptoms return and the swelling recurs.
Papilledema Treatment and Management
Papilledema treatment focuses on lowering intracranial pressure and resolving the underlying cause. Care typically involves an ophthalmologist, a neurologist, and sometimes a neurosurgeon working together.
Medications
If you are taking drugs that raise ICP, your doctor will stop or replace them. Other medications used to treat papilledema include:
- Carbonic anhydrase inhibitors (acetazolamide / Diamox): First-line treatment for IIH. Reduces cerebrospinal fluid production.
- Topiramate: A second-line option, useful when patients also have migraines or seizures. It supports weight loss in IIH as a secondary benefit. If you could become pregnant, talk to your doctor about pregnancy risks and contraception before starting it.
- Furosemide: An adjunct diuretic added when acetazolamide alone is not enough.
- Antibiotics: Used when an infection (such as meningitis or a brain abscess) is the underlying cause.
- Anticoagulants: Used when cerebral venous thrombosis is the cause. They keep the clot from growing and help your body clear the blocked vein over time; they do not break the clot up directly.
- Corticosteroids: Reduce inflammation in inflammatory causes, but starting or stopping steroids is itself a trigger for papilledema in IIH.
- Pain relievers: Acetaminophen and NSAIDs are preferred for headache management. Use opioid pain medications only as directed; routine use is not a standard IIH treatment and contributes to medication-overuse headache.
Surgery
Surgical options for decreasing brain pressure or protecting the optic nerve include:
- Lumbar puncture: Drains cerebrospinal fluid and provides short-term symptom relief
- CSF shunt (ventriculoperitoneal or lumboperitoneal): Redirects cerebrospinal fluid for longer-term ICP control
- Optic nerve sheath fenestration: Relieves pressure on the optic nerve to protect vision when sight is threatened
- Venous sinus stenting: Used in select IIH patients with venous sinus stenosis
- Bariatric surgery: Considered in patients with IIH and obesity when weight loss is part of long-term management
When an abscess or brain tumor is the cause, a neurosurgeon performs burr-hole aspiration, craniotomy, or tumor resection.
When to See a Doctor
- Go to the ER the same day if you have new or recurring vision blackouts (TVOs), double vision, severe or worsening headache with vomiting, or a clinician told you there is optic nerve swelling on exam
- Call your eye doctor or neuro-ophthalmologist promptly for ongoing morning headaches or pulsatile tinnitus when you have no vision symptoms; same-day if vision symptoms appear
- Routine eye exam follow-up is enough if you were told you have a "large optic nerve" or a "full-looking disc" with no symptoms; that is likely physiologic cupping, not papilledema
- Bring a list of all your medications, especially tetracycline antibiotics, isotretinoin, vitamin A supplements, and corticosteroids, because stopping a triggering medication early gives you the best chance of recovery

