

Myopia (nearsightedness) affects an ever-growing segment of the global population. Once seen predominantly as a correctable inconvenience, myopia is now recognized as a major public health concern, especially among children and younger adults.
The steep rise in cases over the past 20 years has prompted worldwide research into its causes, risk factors, and effective interventions. Recent studies indicate that this growth is not uniform across regions or demographic groups.
Many high-income and rapidly urbanizing societies show especially large increases in myopia prevalence. Meanwhile, health experts stress the urgent need for preventive measures, better access to vision correction, and longer-term strategies to slow progression and reduce related risks.
Noteworthy Statistics
- By 2050, approximately half of the global population (close to 5 billion people) may be myopic, with about 10% of all people experiencing high myopia.
- In the United States, prevalence among those aged 12 to 54 rose from about 25% in the early 1970s to over 40% by 2004, reflecting an especially sharp increase among younger cohorts.
- Some East Asian countries report adolescent myopia rates exceeding 80 to 90%, with a few studies showing rates in urban young adults reaching 96% or more.
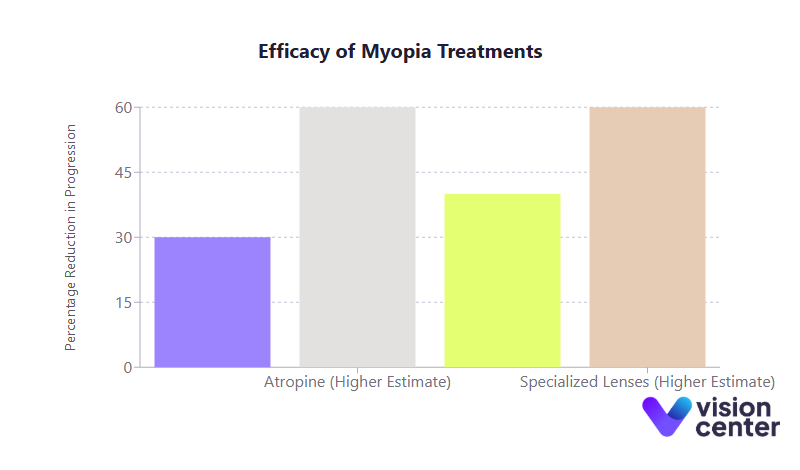
- Low-dose atropine eye drops have shown 30 to 60% efficacy in slowing myopia progression in children, while specialized lenses (e.g., multifocal contacts, orthokeratology) similarly reduce progression rates by 40 to 60% on average.
Understanding the Global Scope of Myopia
Data collected over the last two decades leaves little doubt that myopia has become a critical issue in global eye health. This section examines how prevalence differs across regions, why certain demographic groups appear more at risk, and how these trends have changed over time.
Worldwide Distribution and Regional Differences
- East and Southeast Asia host some of the highest myopia rates in the world, partly attributed to intense educational pressures, high rates of urbanization, and lifestyle factors that encourage prolonged near work.
- High-income regions in Asia, such as Singapore, Taiwan, and South Korea, show myopia prevalence as high as 80 to 90% among teenagers. In South Korea, certain urban surveys suggest that up to 96% of young adults are myopic.
- North America and Europe are also experiencing a rising prevalence. In the United States, the rate of myopia among younger individuals is estimated to have nearly doubled between the early 1970s and the early 2000s.
- Africa generally reports lower prevalence, though more recent data hint at an upward shift as cities grow and lifestyles change.
Prevalence Figures: A Snapshot
| Region/Country | Approximate Myopia Prevalence |
|---|---|
| United States (ages 12–54) | Increased from ~25% in the 1970s to ~41% by 2004 |
| China (urban high school) | ~80% or higher in some urban areas |
| South Korea (urban young adults) | Up to ~96% in certain cohorts |
| Europe | ~20 to 40%, trending upward over the past two decades |
| Global (2020) | ~34% overall, with significant regional variation |
| Global (Projected 2050) | ~50% of the population, with ~10% high myopia |
These numbers highlight how widely myopia prevalence can range, emphasizing the role of environmental and behavioral factors (in addition to genetic predisposition).
Age Group Trends and the “Earlier Onset” Phenomenon
Myopia often starts in childhood and progresses until the eye stops growing, usually in the late teens or early twenties. Alarmingly, many studies show that myopia is both starting at younger ages and reaching higher levels by adolescence than in the past:
- In parts of China, prevalence in first-graders (around age 6) may be under 20%, but it can climb above 70 to 80% by high school.
- In the United States, younger generations are becoming myopic more quickly; Southern California studies revealed a jump from about 15% myopia in early childhood to nearly 60% by late adolescence.
Early onset is concerning because a longer window of progression often results in higher, more severe myopia by adulthood. Healthcare systems worldwide are taking note, focusing on age-specific interventions to prevent or delay onset whenever possible.
Key Risk Factors Driving Myopia
A combination of genetics, environment, and lifestyle choices contributes to the rising rates of myopia worldwide. While genetic predisposition remains relevant, changes in daily habits explain much of the rapid increase over just two or three decades.
Educational Intensity and Near Work
- Prolonged near work, whether reading, studying, or using digital devices, places sustained focusing demands on the eye.
- In regions with highly competitive education systems, students often spend hours each day on close-up tasks. Multiple analyses confirm a correlation between longer schooling and higher myopia prevalence.
- Research using advanced genetic methods indicates that each additional year of education can lead to a more myopic refractive error, suggesting a causal effect beyond simple correlation.
Reduced Outdoor Time
- Modern lifestyles frequently limit time spent outdoors, replacing it with indoor study or recreation.
- Outdoor environments with brighter natural light may help regulate eye growth by stimulating healthy retinal chemical pathways.
- Urban children who spend less than one hour per day outside often show higher myopia rates than their rural counterparts who enjoy more outdoor playtime.
Digital Device Usage
- Widespread availability of smartphones, tablets, and computers has sharply increased daily screen time among both children and adults.
- Some studies find a dose-response relationship: more screen time, higher odds of developing myopia. Screen-based activities compound typical near work and can crowd out beneficial outdoor play.
- Although it can be challenging to separate the impact of “screen use” from near work overall, the COVID-19 era demonstrated that intense digital reliance (often coupled with limited outdoor activity) accelerates myopia progression in young people.
Urbanization and Lifestyle Changes
- Overcrowded, high-rise living conditions in many cities limit the opportunity for distance viewing.
- Urban children may spend substantially more time on academics and screen-based activities compared to rural peers, exacerbating near work exposure.
- This shift is especially clear in countries transitioning from predominantly rural lifestyles to modern urban societies, paralleling the overall increase in myopia prevalence.
Genetic Susceptibility
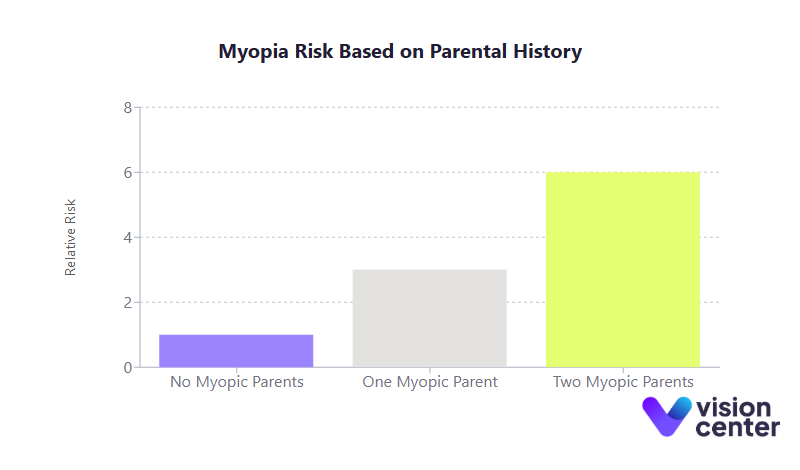
- Children with one myopic parent have roughly triple the risk, and those with two myopic parents about six times the risk, compared to peers with no myopic parents.
- Genetic predisposition alone cannot explain the rapid global surge; rather, the environment often “activates” or amplifies genetic risks.
- Ethnic differences in prevalence also seem heavily shaped by regional lifestyle patterns. Historically low-risk groups have seen large increases in tandem with urbanization and educational changes.
Highlighting Prevention and Intervention Outcomes
Recognizing that myopia typically originates in childhood, much of the current research and public health focus centers on measures to prevent the onset or slow progression in young people. Below are the most prominent strategies and their evidence-based effectiveness.
Increasing Outdoor Time
- A major randomized trial showed that adding 40 minutes of daily outdoor play at school reduced three-year myopia incidence by around 23% compared to controls.
- The protective effect appears greater for preventing myopia from starting than for halting progression in children already myopic.
- Public health campaigns in East Asia and beyond encourage at least two hours of daily outdoor playtime to safeguard children’s vision.
Visual Hygiene and Balanced Lifestyles
- “Visual hygiene” involves taking breaks from close work (e.g., the 20-20-20 rule: every 20 minutes, look 20 feet away for 20 seconds), ensuring good lighting, and maintaining adequate reading distance.
- While hard to quantify precisely, these habits help reduce continuous strain and possibly slow eye elongation.
- Physical exercise and sports, when they replace sedentary near work, are associated with lower myopia risk in observational studies.
Pharmacological Approaches (Low-Dose Atropine)
- Low-dose atropine eye drops (0.01 to 0.05%) have emerged as a top-tier method for slowing myopia progression.
- Studies show a 30 to 60% reduction in progression over a few years, with fewer side effects at lower doses than with older high-dose regimens.
- Higher low-doses (0.05%) tend to offer stronger control than 0.01%, while still minimizing common side effects like light sensitivity.
Special Optical Designs
Innovations in lens design go beyond mere correction, actively targeting myopia control:
- Orthokeratology (Ortho-K): Overnight rigid lenses gently reshape the cornea, often slowing myopia progression by 40 to 60% or more.
- Multifocal Soft Contact Lenses: Designs featuring multiple focusing zones reduce peripheral hyperopic defocus and have shown about 50% slower progression compared to single-vision lenses.
- DIMS Spectacle Lenses: These specialized glasses also create a myopic defocus in peripheral vision, reporting ~52% slower refractive change and ~62% reduced axial elongation over two years.
| Intervention | Approximate Reduction in Myopia Progression |
|---|---|
| Outdoor Time Increase | ~23% fewer new cases (prevention benefit) |
| Low-Dose Atropine Drops | ~30 to 60% slower progression, dose-dependent |
| Orthokeratology (Ortho-K) | ~40 to 60% less axial elongation |
| Multifocal Contacts | ~50% lower progression (over 2–3 years) |
| DIMS Spectacle Lenses | ~50 to 60% slower refractive change/eye growth |
While none of these measures fully stop progression for every child, deploying them early can markedly reduce the final severity of myopia. Experts often combine two or more strategies (e.g., atropine plus specially designed contact lenses) for enhanced effect.
Conventional Vision Correction and Refractive Surgery
- Single-vision glasses or standard contact lenses correct myopia but generally do not slow progression.
- Laser refractive surgery (e.g., LASIK, PRK, SMILE) can permanently correct established myopia in adults, with over 90% of LASIK recipients achieving 20/20 vision.
- Surgery, however, does not address the underlying risk of future eye complications from high myopia if the eye continues to elongate. Consequently, it is not an option for children and teens still progressing.
Broader Consequences: Quality of Life, Economic Burden, and Education
Quality of Life and Vision Health
- Most mild or moderate myopia is easily remedied with corrective lenses, mitigating daily life disruption.
- High myopia (often defined as worse than –6.00 D) carries greater dependence on thick lenses or specialty contacts and significantly raises the risk of retinal detachment, myopic maculopathy, glaucoma, and other severe eye conditions.
- Individuals with high myopia often report reduced vision-related quality of life, citing issues ranging from social stigma to anxiety over possible sight-threatening complications.
Educational and Social Impacts
- On the one hand, intensive education is associated with higher myopia rates due to near work and less time outdoors.
- On the other hand, uncorrected myopia hinders classroom learning. Studies in rural schools demonstrate improved test scores and even reduced dropout rates once children receive appropriate eyeglasses.
- Children with severe, uncorrected myopia may limit extracurricular participation or develop self-esteem challenges. Correction typically alleviates many of these barriers, emphasizing how crucial access to vision care is for educational outcomes.
Economic Costs and Lost Productivity
- Routine expenses for eye exams, glasses, contact lenses, and potential surgeries can total billions of dollars annually in nations with high myopia rates.
- Uncorrected myopia remains a driver of lost economic productivity worldwide: an estimated $200+ billion in annual productivity losses are linked to people who lack access to proper vision correction.
- High myopia also translates into higher rates of serious eye disease. Long-term care for retinal or macular problems significantly increases healthcare costs.
- In countries where military service or certain occupations demand clear unaided vision, widespread myopia can diminish recruitment pools and reduce workforce participation in specific fields.
Global Trends: Looking Ahead
Despite growing awareness, myopia prevalence continues to climb in many parts of the world. Experts warn that, if current patterns persist, nearly 50% of the global population may be myopic by mid-century. This includes a significant fraction developing high myopia, heightening the risk of irreversible vision loss later in life.
Regional Developments
- East Asia: Already experiencing extreme rates of myopia among youth. Some policy interventions (e.g., mandated outdoor classes in China and Singapore) aim to stem the tide.
- North America and Europe: While not at East Asian levels, both regions note a substantial uptick in recent decades. Public health initiatives encourage less screen time and more outdoor activity, though systemic changes can be slow.
- Developing Regions: As rapid urbanization and educational expansion continue, more children in Africa, South Asia, and Latin America may adopt the near-work-heavy lifestyles associated with myopia’s rise.
Potential Future Measures
- School-Based Programs: Mandatory outdoor breaks, “bright classrooms” that mimic outdoor light intensity, and routine vision screenings have shown promise in controlling onset rates.
- Emerging Treatments: Further refinements to atropine formulations, new types of myopia-control lenses, and potential pharmaceutical breakthroughs might strengthen the efficacy and comfort of slowing eye growth.
- Technology Solutions: Smartphone apps and wearable devices could guide children to take appropriate breaks, maintain correct reading distances, and track daily outdoor exposure.
- Global Collaboration: International coalitions such as the International Myopia Institute (IMI) are promoting standardized guidelines and encouraging cross-border research and data sharing.
Ultimately, effective myopia management requires public health strategies, not just clinical treatments in isolated settings. The hope is that consistent efforts to address near-work habits, protect outdoor playtime, and provide early interventions can flatten or reverse the current trajectory.
In summary, data gathered over the past two decades underscore the dramatic spread of myopia worldwide, well beyond any single region or demographic. As more children spend large portions of their day indoors and are focused on close-up tasks, earlier onset and faster progression become increasingly common.
Public health initiatives, advanced lens technologies, and pharmacologic solutions offer hope for bending this curve. Each approach has a documented capacity to reduce the rate of progression or delay onset.
Addressing this global concern will likely require multifaceted cooperation among policymakers, educators, eye care professionals, and families. The reality that half of humanity could soon be myopic underscores an urgent need for sustained attention. Collaborative action today can ensure that the “myopia boom” does not translate into a crisis of avoidable vision impairment tomorrow.

