

Vision rehabilitation helps individuals with uncorrectable vision loss maximize their remaining sight and improve day-to-day independence. In the United States, these programs have demonstrated notable success in mitigating the functional and emotional toll of low vision, particularly among older adults.
Over the last decade, multiple studies have tracked the efficacy of vision rehabilitation, highlighting improvements in overall visual function, activities of daily living, and quality of life.
Stakeholders in public health and healthcare policy increasingly see rehabilitation as a cost-effective strategy to help people maintain independence, reduce healthcare expenditures, and stay engaged in their communities.
Key Statistics at a Glance
- Clinically Meaningful Improvement: In one large multi-center study, 47% of adults achieved clinically significant gains in overall visual ability within 6 to 9 months of starting a low-vision rehabilitation program.
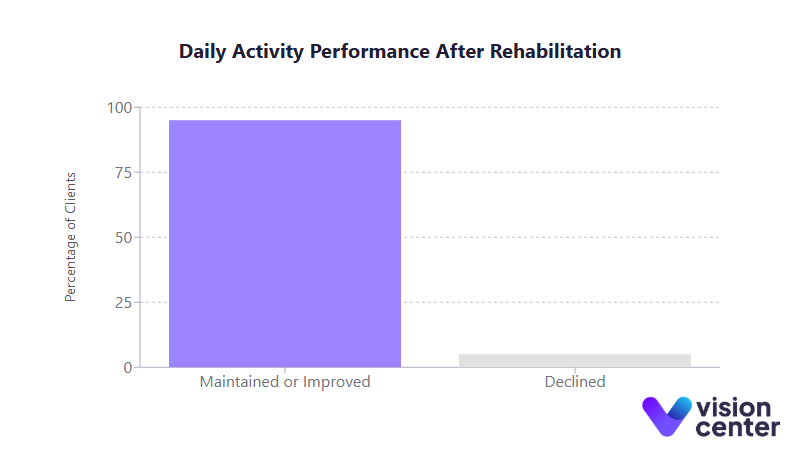
- High Independence Rates: A community-based program reported that 95% of its clients either maintained or improved their ability to carry out essential daily activities following rehabilitation services.
- Economic Burden: The annual cost of vision loss in the United States exceeds $130 billion, underscoring the potential savings that effective rehabilitation can bring by preventing falls, deferring nursing home admissions, and enabling workforce participation.
- Insurance Gaps: Medicare and most private insurers do not cover low-vision devices (e.g., magnifiers, adaptive eyewear), which can limit access to tools that significantly improve patients’ functional outcomes.
Understanding Vision Rehabilitation Services
Vision rehabilitation offers systematic training and support for individuals whose vision cannot be corrected by standard glasses, surgery, or other medical interventions. This approach includes:
- Evaluation by low-vision specialists to determine the extent of impairment and specific challenges.
- Adaptive device training for magnifiers, screen readers, or closed-circuit television systems that enlarge print and images.
- Orientation and mobility (O&M) instruction to help individuals navigate environments safely.
- Occupational therapy sessions covering reading, cooking, self-care, and medication management techniques.
- Psychosocial support aimed at addressing the emotional impact of vision loss.
Vision loss frequently leads to decreased independence, higher fall risk, and significant emotional distress if left unaddressed. By providing tailored strategies, rehabilitation programs improve both daily functioning and quality of life.
Program Effectiveness and Outcome Trends
Vision rehabilitation programs have consistently demonstrated the ability to stabilize or improve individuals’ functional capabilities. This section highlights why these data points are crucial for gauging the real-world impact on those living with visual impairments.
- Outpatient Clinics: A multi-center study of hundreds of adult patients found that nearly half experienced a clinically meaningful boost in overall visual function within months of attending an outpatient low-vision rehabilitation clinic. Gains were seen in reading, mobility, and other daily tasks. Equally significant, individuals who did not receive rehabilitation often experienced a decline in their abilities over the same period.
- Intensive Inpatient Programs: Veterans Affairs (VA) Blind Rehabilitation Centers offer immersive 4- to 6-week programs with daily training, reporting especially high success rates. Studies suggest that intensive residential services can lead to greater improvements in visual ability compared to typical outpatient visits, highlighting how higher-frequency instruction can accelerate skill development.
- Community-Based Agencies: In some regions, nonprofits and local rehabilitation centers coordinate services, conduct home visits, and provide device loan programs. One notable example documented a 95% “success rate” in helping participants maintain or enhance their day-to-day independence. This measure typically tracked performance in core living activities, from personal care to household tasks.
- Emerging Tele-Rehabilitation: As telehealth infrastructure grows, remote consultation and device training have become more accessible. Early program data show promise for patients who have limited access to specialized clinics, though large-scale trials are still in progress.
Common Factors That Influence Rehabilitation Outcomes
- Training Duration: Whether condensed into an intensive month or spread over several outpatient visits, having a sufficient “dose” of training is strongly linked to meaningful improvements.
- Comprehensive Services: Programs that combine assistive technology instruction with counseling, orientation and mobility, and caregiver education tend to yield the highest success rates.
- Device Provision: Obtaining the right low-vision devices and learning to use them properly can dramatically enhance rehabilitation outcomes.
- Follow-Up and Reinforcement: Many organizations recommend periodic check-ins to address changing vision needs over time, ensuring that patients retain and refine their newly learned skills.
Patient Demographics and Participation
Collecting demographic data helps providers and policymakers identify gaps in service access and tailor rehabilitation approaches to specific populations. Understanding who seeks vision rehabilitation and who may still be underserved plays a key role in ensuring equitable care.
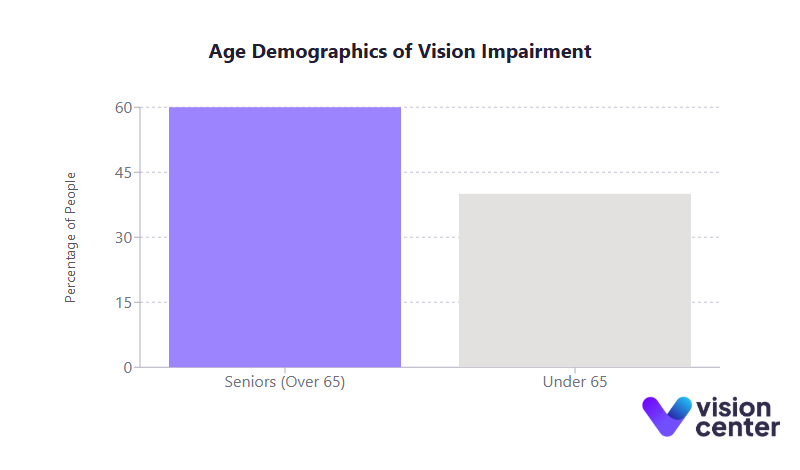
- Older Adults: Around 60% of Americans with significant vision impairment are seniors over age 65. Not surprisingly, most vision rehab clients are 70 or older, often dealing with age-related macular degeneration, glaucoma, or diabetic retinopathy.
- Gender: Because women generally live longer and have higher rates of age-related eye diseases, they represent a slight majority of rehabilitation participants.
- Racial/Ethnic Disparities: In absolute numbers, non-Hispanic White adults form the largest group with vision impairments. However, data indicate African American and Hispanic adults have a higher per-capita risk of vision loss and often face greater barriers to care. These disparities translate into fewer minorities seeking or receiving vision rehabilitation services.
- Socioeconomic Status: Vision loss frequently correlates with lower incomes and limited education. Cost barriers, particularly the lack of insurance coverage for devices, can deter many low-income individuals from completing rehabilitation programs. Charitable support or grants that offset equipment costs have proven helpful in bridging this gap.
- Geographic Patterns: Populous areas usually have more rehabilitation resources, while rural regions often lack specialized services. States with older demographics, such as Florida, have higher rates of severe vision impairment, emphasizing the need for accessible local programs.
| Demographic Factor | Key Insights |
|---|---|
| Age | Seniors comprise the majority (60+%). Demand for rehab rises with conditions like AMD. |
| Gender | Women slightly outnumber men in rehabilitation usage, partly due to longevity trends. |
| Race/Ethnicity | Minority groups experience higher per-capita risk of vision impairment yet face coverage and referral barriers. |
| Socioeconomics | Lower-income individuals often have difficulty affording assistive devices and therapy. |
| Geography | Rural areas may have few low-vision specialists, leading to reliance on tele-rehab or traveling. |
Functional Gains and Quality of Life Improvements
One of the most vital aspects of rehabilitation is its measurable impact on day-to-day living and overall well-being. These data illuminate the far-reaching benefits of structured low-vision services.
- Daily Activities: Many patients regain or significantly enhance their ability to read, manage finances, cook, recognize faces, and navigate indoor and outdoor environments. In various outcome studies, upwards of 90% reported notable improvements in at least one crucial daily activity.
- Independence: Sustaining or boosting personal independence can allow older adults to remain in their homes rather than transition to assisted living. Independence also fosters a sense of dignity and reduces reliance on caregivers or family members.
- Mobility and Falls: Orientation and mobility specialists teach effective cane techniques, spatial awareness, and safe travel skills. These interventions often lead to fewer falls, reducing injury costs and hospitalization rates among older adults with low vision.
- Mental Health: Depression and anxiety rates drop when individuals receive rehabilitation. Regaining the ability to perform everyday tasks independently often restores confidence, lowers emotional distress, and promotes social engagement.
- Employment (Working-Age Adults): Nationally, less than half of working-age adults with serious vision impairments are employed, a stark contrast to the general population’s employment rates. However, vocational rehabilitation services show a track record of helping individuals retain or gain employment, thereby improving financial independence and quality of life.
Economic Impact and Cost-Benefit Analysis
Vision loss exacts a substantial financial toll on both individuals and the healthcare system. Understanding these costs highlights why effective vision rehabilitation is not just beneficial for patients but also economically prudent.
- Overall Annual Costs: Recent estimates place the yearly economic burden of vision loss in the United States at well over $130 billion. This encompasses direct costs like medical care and long-term nursing, plus indirect costs such as lost productivity and informal caregiver time.
- Projected Growth: As the population ages, forecasts indicate that total annual costs could rise to $385 billion by the early 2030s and potentially surpass $700 billion by mid-century.
- Cost Per Person: On average, each person with vision impairment can incur nearly $17,000 annually in combined direct and indirect expenses, reflecting medical bills, assistive care, and employment challenges.
- Rehabilitation vs. Long-Term Care: While comprehensive low-vision rehab might cost a few thousand dollars per patient, it can forestall the need for nursing home placement that can cost tens of thousands of dollars per year. Even reducing the likelihood of a single fall-related hospital visit can offset a large portion of a rehabilitation program’s costs.
- Return on Investment: Multiple analyses, including cost-utility studies, suggest that when measured in “cost per Quality-Adjusted Life Year,” vision rehabilitation falls into a highly cost-effective category, especially compared to the expenses of untreated or poorly managed vision loss.
| Economic Metric | Approximate Value (USD) |
|---|---|
| Annual total cost of vision loss | $130+ billion |
| Average yearly cost per affected person | $16,000 to $17,000 |
| Projected annual cost by 2032 | $385 billion |
| Projected annual cost by 2050 | $700+ billion |
| Falls/injury-related excess medical costs | $500 million+ |
Insurance Coverage and Funding Landscape
How rehabilitation services are funded can significantly affect patient access and outcomes. While the evidence strongly supports the benefits of vision rehab, coverage barriers remain.
- Medicare: Medicare Part B covers occupational therapy for vision rehabilitation if a physician prescribes it, but it excludes coverage of low-vision devices like specialized magnifiers. This gap forces many seniors to pay out of pocket for the very tools that can yield the largest functional gains.
- Private Insurance: Most private plans mirror Medicare in not covering assistive devices. Some do pay for a limited number of OT sessions, but coverage is inconsistent.
- Medicaid: States vary widely in their vision benefits. Some Medicaid programs include limited coverage for rehabilitation services and basic assistive devices, especially for children or adults with multiple disabilities. Others provide minimal benefits, making philanthropic or nonprofit programs critical.
- Veterans Affairs (VA): A fully integrated model exists within the VA system, which provides comprehensive coverage of therapy, devices, and even travel to specialized blind rehabilitation centers. Studies consistently show that this model achieves higher success rates thanks to seamless funding and availability of assistive technologies.
- Nonprofit and Community Support: Many individuals rely on charitable grants, device loan programs, or state commissions for the blind to fill coverage gaps. This patchwork approach varies by region, leaving some areas with limited resources.
Tables and Visual Data Presentation
Data from numerous outcome reports demonstrate strong evidence for the effectiveness of vision rehabilitation:
| Program Model | Sample Outcomes |
|---|---|
| Outpatient Clinics | Around half of participants achieve clinically meaningful improvement in reading, mobility, or daily tasks. |
| Inpatient VA Centers | Effect-size measures significantly favor immersive, concentrated training with device costs covered. |
| Community Agencies | Some record 90%+ of clients sustaining or increasing independence in activities of daily living. |
| Tele-Rehab Programs | Early feedback is positive for homebound or rural patients, though large-scale efficacy data are still emerging. |
These programs can help individuals retain or regain critical life skills by combining consistent training schedules, assistive device provision, psychosocial support, and appropriate insurance coverage.
Final Thoughts
Vision rehabilitation statistics from the past decade highlight key successes in improving functional outcomes and maintaining independence for those living with low vision. Multi-center studies and community program data consistently show that a significant portion of participants achieve clinically meaningful gains in mobility, self-care, and reading ability. These improvements can also help relieve the burden on caregivers and reduce fall-related injuries, creating a ripple effect of benefits that extend beyond individual patients.
At the same time, many Americans face uneven access to these services. Insurance limitations, out-of-pocket device costs, racial/ethnic disparities in care, and shortages of trained professionals all hinder broader adoption. Yet the data underscore a strong economic case for expanding coverage and availability.
Where robust rehabilitation is delivered, participants often see long-lasting improvements in both daily function and emotional well-being. Strengthening referral pathways, building telehealth solutions, and revisiting coverage policies for essential low-vision devices stand out as pivotal steps toward more equitable and effective care.
Looking ahead, as the aging population grows and the incidence of chronic eye diseases increases, vision rehabilitation will likely play an even more critical role in public health strategies. Ongoing research into tele-rehabilitation, advanced assistive technologies, and cost-effectiveness could open the door to broader, more inclusive services. Ultimately, these statistics reaffirm the transformative potential of comprehensive low-vision rehabilitation, helping individuals lead fuller, safer, and more autonomous lives.

