

Eye disease affects millions across the United States, yet not all communities experience the same risks, care opportunities, or outcomes. Understanding the statistical landscape of eye conditions across different ethnic groups is crucial for targeting interventions that prevent needless vision loss and promote equitable healthcare.
Over the past decade, studies from federal agencies, medical associations, and vision research initiatives have revealed enduring differences in disease prevalence, access to eye care, and treatment outcomes among major racial and ethnic groups.
These disparities underscore the need for improved awareness, accessible screening programs, and tailored healthcare solutions, especially for communities most impacted by conditions such as glaucoma, diabetic retinopathy, and age-related macular degeneration.
Below are several especially notable statistics that set the stage for a deeper discussion:
- Glaucoma prevalence is 3 to 4 times higher in Black Americans compared to White Americans, leading to a greater risk of blindness in this population.
- Diabetic retinopathy has doubled nationally since 2004, with Black and Hispanic individuals facing the highest rates of vision-threatening stages.
- Cataract surgery uptake is significantly lower in Black and Hispanic seniors compared to White seniors, contributing to higher rates of preventable cataract-related vision loss.
- Age-related macular degeneration (AMD) occurs most frequently among White Americans (particularly in older age groups), while Black and Hispanic populations have relatively lower AMD prevalence but higher burdens of glaucoma and diabetic eye disease.
Overview of Ethnic Disparities in Eye Disease
Disparities in eye disease are intertwined with broader social and health factors. African Americans and Hispanic/Latino populations are disproportionately affected by conditions such as glaucoma and diabetic retinopathy, partly reflecting elevated rates of hypertension, diabetes, and limited access to preventive care.
Meanwhile, White Americans have the highest incidence of age-related macular degeneration, linked in part to gene variants common in European ancestry. Although modern treatments can effectively manage or even prevent many forms of blindness, longstanding inequalities in insurance coverage, healthcare access, and early detection often result in worse vision outcomes among minority groups.
Prevalence Patterns and Core Statistics
Understanding how common each condition is among different ethnicities helps identify who is most at risk. This knowledge also informs resource allocation for screening and education.
- Glaucoma
- Black Americans have a glaucoma prevalence estimated to be 3 to 4 times higher than that of White Americans, making glaucoma the leading cause of irreversible blindness in African American communities.
- Hispanic Americans show a similarly high glaucoma prevalence, often catching up to Black Americans in older age brackets (60+).
- Diabetic Retinopathy (DR)
- The number of Americans with vision-threatening diabetic retinopathy has roughly doubled since 2004, driven mostly by higher diabetes rates in minority populations.
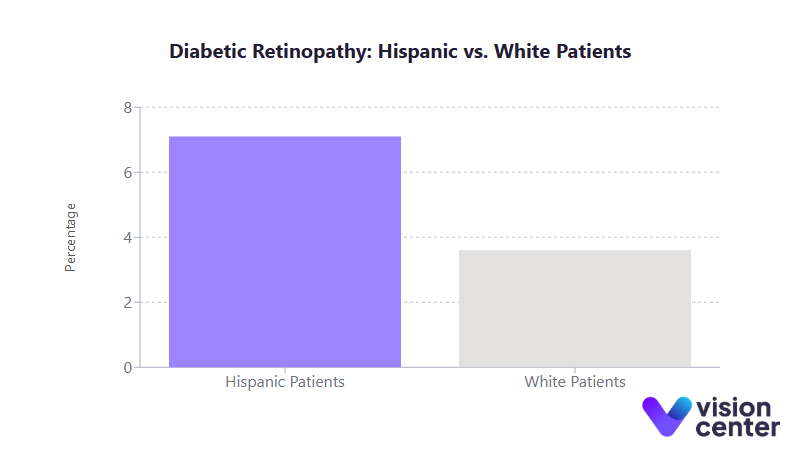
- Black patients have an 8.7% rate of vision-threatening DR among those with diabetes, more than double the rate for White patients, who stand at 3.6%. Hispanics, at about 7.1%, also face significantly higher risks than White diabetics.
- Age-Related Macular Degeneration (AMD)
- AMD remains most prevalent in White populations, who comprise an overwhelming majority of AMD cases nationwide.
- Genetic studies indicate that certain risk variants (e.g., in the CFH gene) are more common in individuals of European descent, aligning with AMD’s disproportionately high rates in White seniors.
- Cataract
- By age 80, over half of all Americans develop cataracts, with the absolute highest numbers found in older White adults.
- Nevertheless, Black and Hispanic communities often experience later surgical intervention and potentially more advanced disease before treatment, indicating a gap in timely care.
Factors Driving Disparities
The reasons behind these differences in disease burden are multifaceted, spanning genetics, systemic health conditions, and social determinants.
- Genetic Susceptibilities
- European ancestry genes strongly correlate with AMD risk, while African ancestry correlates more strongly with open-angle glaucoma.
- Even when certain risk genes appear in both Black and White populations, such as CFH alleles for AMD, other genetic or environmental factors seem to protect one group or elevate risk in another.
- Co-Existing Health Conditions
- Higher rates of diabetes and hypertension in Black and Hispanic groups exacerbate diseases like glaucoma and retinopathy.
- Smoking rates, historically higher in some White populations, have contributed to greater AMD prevalence.
- Socioeconomic and Access Barriers
- Cost, insurance coverage, and provider availability influence who gets routine exams. Many communities of color lack easy access to ophthalmologists or optometrists.
- Even with Medicare, minority seniors are less likely to undergo sight-preserving procedures such as cataract surgery at earlier, more treatable stages.
Treatment Responses and Outcomes
Modern treatments for serious eye conditions, whether surgical procedures, medications, or laser therapy, are typically effective across all racial and ethnic groups in a purely clinical sense. Disparities emerge primarily due to differences in disease stage at diagnosis and the consistency of follow-up:
- Glaucoma
- Black patients are more likely to present with advanced visual field damage and are about six times more likely to experience severe vision loss even after initiating standard treatments.
- Hispanic patients similarly face advanced presentation, although comprehensive data suggests they fall between Black and White patients in treatment timing and outcomes.
- AMD Therapies
- Anti-VEGF injections have cut the incidence of blindness from neovascular AMD by as much as 50% among White Americans.
- Minorities with AMD benefit similarly when treated, but they are significantly less likely to receive timely anti-VEGF injections, reflecting both underdiagnosis and access issues.
- Diabetic Retinopathy Management
- Laser photocoagulation and anti-VEGF for diabetic macular edema can preserve vision in most patients. However, high-risk minorities commonly present late and may not receive the necessary interventions early, contributing to elevated rates of blindness from diabetes.
- Cataract Surgery
- More than 95% of patients experience improved vision after cataract extraction, regardless of ethnicity.
- Due to cost or limited healthcare navigation, Black and Hispanic patients tend to delay surgery longer, sometimes until the cataract is hyper-mature, reducing the likelihood of optimal post-operative outcomes.
Access Disparities in Eye Care
Routine screening and preventive exams are central to managing eye disease, but utilization differs markedly among ethnic groups.
- Routine Exams
- About 58 to 60% of White adults at high risk for vision loss report seeing an eye care provider annually, compared to roughly 50 to 55% of Black and Hispanic adults.
- Among working-age adults with diabetes, minority communities have shown declining annual exam rates over certain periods, whereas White populations have seen incremental improvements.
- Financial and Insurance Barriers
- Cost is a frequent obstacle, with a higher percentage of Black and Hispanic patients unable to afford eyeglasses, let alone specialty procedures.
- Many rely on Medicaid, which often provides narrower coverage for comprehensive eye exams and diagnostic testing compared to private insurance.
- Geographical Limitations
- Vision care “deserts” exist in rural and underserved urban areas, affecting minority neighborhoods disproportionately.
- Limited public transportation and a lack of bilingual services for Spanish-speaking communities can further compound the accessibility challenge.
Prevention Program Effectiveness
Preventive efforts aim to reduce barriers to care and raise awareness about early intervention:
- Community Initiatives
- Church-based glaucoma workshops, Spanish-language diabetes education, and local screening events have improved knowledge levels. However, actual exam rates and adherence do not always rise proportionally.
- Telehealth screening in primary care clinics shows promise for bridging gaps in places where eye specialists are scarce.
- School and Childhood Screenings
- Providing free glasses in predominantly minority school districts significantly reduces uncorrected refractive errors.
- Despite these gains, large numbers of children who fail vision screenings in low-income districts still do not receive follow-up exams or corrective lenses.
- Outcome of Screening Programs
- Early evidence from some Hispanic communities suggests that on-site diabetic retinopathy screening can slow progression to blindness by catching disease sooner.
- Similarly, initiatives targeting African American families have prompted more relatives of glaucoma patients to seek screening, modestly lowering rates of undiagnosed disease.
Utilization Trends by Ethnicity
Overall eye care usage remains uneven, shaped by both cultural perceptions and systemic obstacles:
- Preventive vs. Reactive Visits
- White Americans typically have more routine checkups, while Black and Hispanic patients often seek care only if symptoms become pronounced.
- As a result, diseases like glaucoma or diabetic retinopathy may be identified at later, more vision-threatening stages among minority groups.
- Medicare Populations
- Even among seniors who share uniform federal insurance, cataract surgery rates have historically been 30% lower in Black beneficiaries.
- Blacks with glaucoma often require more frequent follow-up visits, reflecting greater disease severity once they enter the care system.
- Regional Variations
- Some states with robust public health initiatives report better minority screening rates, while others, especially where provider shortages intersect with poverty, continue to struggle in bridging gaps.
Persistent Outcome Disparities
Despite broad medical advances, outcome differences remain stark:
- Higher Blindness Rates
- African Americans consistently show the highest prevalence of blindness among major ethnic groups, largely driven by glaucoma and cataracts left untreated for too long.
- Hispanic communities, particularly those with high diabetes rates, see increasing cases of diabetic retinopathy–related blindness.
- Worse Final Vision
- In glaucoma, for example, up to 15% of Black patients in certain large studies progressed to legal blindness at final follow-up, compared to about 5% of White patients.
- Earlier diagnosis and continuous care reduce blindness risk, but such continuity is far less accessible in many minority neighborhoods.
- Quality of Life Impacts
- Black and Hispanic patients report worse vision-related quality of life at comparable clinical stages, partly due to limited use of low-vision aids and rehabilitation services.
- Cultural, linguistic, and financial barriers further impede access to the adaptive tools needed to remain independent when eyesight declines.
Intervention Success Rates
Eye care interventions have had a transformative effect on public health, though the benefits do not always spread evenly:
- Cataract Surgery
- Nationwide, it has achieved a 40 to 50% reduction in moderate vision impairment among older Americans in recent decades.
- Lower uptake in minority groups, however, means these communities have not experienced equal levels of improvement.
- Anti-VEGF Therapies
- These injections have halved the incidence of blindness from wet AMD among populations who receive them regularly.
- The success rate is similarly high for diabetic macular edema, but lower treatment adherence among minorities offsets the full benefits.
- Laser Treatments
- Pan-retinal photocoagulation for proliferative diabetic retinopathy lowers the five-year risk of blindness by over 50%.
- Delayed detection and variable follow-through still result in disproportionately high rates of severe retinopathy in African American and Hispanic communities.
Long-Term Outlook
Demographic shifts indicate that the number of older adults, particularly in Hispanic and Black populations, will continue to rise. Consequently:
- Growing Burdens
- By 2050, Hispanics are projected to have the highest prevalence of visual impairment and blindness, as their population ages. Black Americans also remain at heightened risk, especially for glaucoma-driven vision loss.
- White Americans will still see a large absolute number of AMD cases but may benefit most from advanced therapies, continuing to reduce their AMD-related blindness rates.
- Mixed Progress
- Some interventions have narrowed the gap, for instance, increased glaucoma awareness in African American communities, while others show persistent disparities in real-world care.
- Ongoing improvements in telemedicine, combined with culturally tailored programs and expanded insurance coverage, could further reduce late-stage disease by enabling earlier detection.
- Preventive Strategies
- Early screening, comprehensive diabetes management, and routine eye exams remain critical to slowing or halting the progression of diseases that threaten sight.
- Policy efforts aimed at improving healthcare accessibility, language services, and cost support will help ensure new innovations reach every community in need.
In all, the data point to both progress and challenges. Significant breakthroughs in treatment have the power to diminish blindness, yet disparate rates of insurance coverage, routine exam access, and timely follow-up keep many minority groups at higher risk. The next ten years will be pivotal in seeing whether targeted outreach and technology can more fully address these inequalities.
Over the past decade, it has become increasingly evident that our health system must adapt to the growing and diversifying population at risk for eye diseases. Large-scale interventions are vital. Keeping pace with demographic and epidemiological shifts will require sustained commitment from policymakers, healthcare providers, and community stakeholders alike.
By investing in equitable and culturally attuned preventive strategies, the nation can harness advancements in medical science to ensure that fewer people, regardless of background, face preventable vision loss. While the statistics illustrate the urgency, they also highlight the tremendous potential: with timely care, early detection, and ongoing research, we have the tools to preserve sight for millions of Americans in the years ahead.

